|
As you noted in our January 2015 issue of Contact Lens Spectrum, we designated beauty enhancing contact lenses to be the contact lens event of
2014 (http://www.clspectrum.com/articleviewer.aspx?articleID=112120). For a
variety of reasons, the �cosmetic� contact lens segment of the market has remained stagnant for many years. We anticipate that the new technologies in this
space will allow for some increased enthusiasm and expansion of this market segment. We would like to get your thoughts on this. Please let us know how you
see the cosmetic category fitting into your contact lens practice in the years to come by emailing us at cltoday@pentavisionmedia.com.
|

|
The Third International Association of Contact Lens Educators (IACLE) World Congress on Contact Lens Education will be hosted by the University of
Manchester, UK, on May 24-28, 2015.
The theme for the congress is Shaping the Future of Contact Lens Education. Delegates will hear experts from a wide range of backgrounds
explore technologies and approaches that can be applied to contact lens teaching. Sessions will also be broadcast live online as Web Lectures for IACLE
members around the world to take part.
Keynote speakers and topics include:
-
Dr. Helen Crompton, Assistant Professor of Instructional Technology at Old Dominion University Virginia, USA, who will review the latest and future
educational technologies such as augmented reality, wearable technologies and robotics.
-
Apple Distinguished Educator Joe Moretti, who will look at the iPad as a powerful mobile tool for explaining concepts and nurturing
understanding, and for creating electronic books to distribute to students.
-
Professor Patrick Caroline of the Pacific University College of Optometry in Oregon, USA, will share his expertise in inspiring optometric students and
demonstrating the importance of �life-long learning�.
The program will also feature a special symposium discussing �How can educators grow contact lens penetration around the world?�
Around 100 delegates are expected to attend the Congress, including educators from IACLE�s three global regions: Asia Pacific, Americas and Europe/Arica �
Middle East. Participation for IACLE members will be facilitated by IACLE, thanks to the generous support of Platinum Sponsors Alcon,
CooperVision and Johnson & Johnson Vision Care. In addition to IACLE members, delegates will attend from the Association of Optometric Contact Lens
Educators (AOCLE) and British Universities Committee of Contact Lens Educators (BUCCLE).
For information visit www.iacle.org.
|
|
The GP Lens Institute webinar series has been highly successful the last two years. The remaining 2015 schedule is listed below and represents a very good
blend of specialty GP lenses (i.e., scleral, multifocal, corneal reshaping), lens care, practice management, and custom soft lenses. These presentations
will be given by GPLI Advisory Board members who are considered experts in the specific topic(s) they will be presenting.
For more information, visit www.GPLI.info.
February 17: Specialty Contact Lens Care: Susan Gromacki, OD
March 17: Scleral Lens Fitting for Healthy Eyes: Astigmatic and Presbyopic Applications: Melissa Barnett, OD and Stephanie Woo, OD
April 21: GP and Custom Soft Multifocal Lens Update 2015: Doug Benoit, OD
May 19: �1 - 2 - 3 GP" Corneal Reshaping, Scleral Lenses, and Multifocal Fitting and Applications: Michael Lipson OD
June 16: Hybrid and Piggyback Patient Selection, Fitting, and Troubleshooting: Barry Eiden, OD and Jeff Sonsino, OD
July 21: Ocular Surface Considerations for Custom Contact Lens Care: Mile Brujic, OD and Dave Kading, OD
August 18: Custom Soft Lens Update: Susan Resnick, OD
September 15: How to Effectively Promote and Market Your Specialty Contact Lens Practice: Roxanna Potter, OD
October 20: Myopia Control 2015: Jeff Walline, OD, PhD
November 17: Specialty GP Applications: 1) Fine-tuning Scleral Lens Fits, and 2) Building Your Cornea Reshaping Lens Practice: Jason Jedlicka, OD
December 15: Contemporary Scleral Lens Applications: 1) In Ocular Surface Disease and 2) Lens Care: Michael Ward, FCLSA, FAAO
One hour of CE credit (COPE approved) through the University of Houston is available for various archived webinars. Visit www.GPLI.info to apply and
request your tests.
|
|
Accu-Lens, Inc. announced their newest option in scleral designs, a Dual-Aspheric Multifocal. Accu-Lens�s proven Clarity Plus Multifocal optics is now
available in all their scleral designs including the Maxim and Easy Fit lenses. According to the company, this option provides improved contrast and
clarity of vision throughout a full range of focal points, as well as maintains the corneal integrity.
More information is available at www.acculens.com.
|
|
The Commission on Paraoptometric Certification (CPC), the paraoptometric certifying body of the American Optometric Association, announced that The
Certified Paraoptometric Technician (CPOT) Clinical Examination is now available in a convenient computer-based format. Designed to be widely accessible to
paraoptometrics throughout the year, this exam provides professionals even more opportunities to advance their career in the field of optometry.
The CPOT Clinical exam is offered at more than 200 locations across the United States and Canada four times per year during two-week testing periods held
in February, May, August and November. The new examination incorporates photos and videos into the 100 multiple-choice questions. Award of the CPOT
designation is dependent on candidates successfully completing the CPOT written exam and the CPOT Clinical exam.
To find exam dates and registration deadlines for the CPOT examination, click here. For more information about
all levels of certification for paraoptometrics, visit aoa.org/paraoptometrics, or contact the CPC at CPC@aoa.org or call toll-free, (800) 365-2219, ext. 4210.
|

|
|
|
|
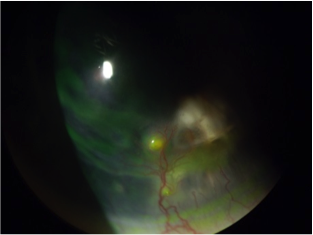
This image shows neo-vascularization onto transplanted cornea due to a broken suture. The suture was removed and the eye was placed on an
antibiotic/steroid regimen after which the eye was refit with a scleral lens.
We thank Dr. Boshnick for this image and we welcome photo submissions from our other readers! It is easy to submit a photo for consideration for publishing
in Contact Lenses Today. Simply visit http://www.cltoday.com/upload/upload.aspx to upload
your image. Please include an explanation of the photo and your full name, degree or title and city/state/country.
^ Back to top
|

|
Quality of Life Issues with Contact Lens Treatments for Keratoconus�Where Do We Start and Where Are We Going?
Our approach to the contact lens management of keratoconus patients often focuses squarely on visual acuity outcomes. The mainstay of such management has
been achieved typically with the use of corneal rigid gas permeable contact lenses due to their ability to mask significant corneal irregularity and
provide dramatically improved visual acuity when compared to spectacles. However we need to remain cognizant of the impact our treatments have on our
keratoconic patient�s quality of life.
A study was recently conducted that evaluated the impact of rigid gas-permeable (RGP) contact lenses on vision-related quality of life (VR-QOL) in
keratoconic patients with different grades of severity.1 Forty-six patients with bilateral keratoconus were divided into three groups according
to the average of the steep keratometry (K) readings in the two eyes of each patient. Main outcome measures included binocular visual acuity (VA), lens
wearing time, the 25-item National Eye Institute Visual Function Questionnaire (NEI-VFQ-25), foreign body (FB) sensation, comfort and overall satisfaction.
Results found that patients with severe keratoconus showed significantly reduced wearing time compared with the other two groups (4.8 � 2.5 hours per day).
Regarding the subjective criteria, there was no significant difference on NEI-VFQ-25 scores, foreign body sensation, comfort and overall satisfaction
between mild and moderate keratoconus groups but scores in the group with severe keratoconus were significantly lower than the other two groups. Binocular
VA strongly correlated with NEI-VFQ-25 scores; however, NEI-VFQ-25 scores had no significant correlations with different disease severities.
The researchers concluded that appropriate correction with RGP lenses contributes to good vision related quality of life for keratoconic patients; however,
as the disease progresses to a steep keratometric value of more than 52 diopters (6.50 mm), RGP lenses did not guarantee a relatively good VR-QOL and other
subjective quality of life measures such as comfort and overall satisfaction with CLs diminish significantly in more advanced disease. They suggested that
alternative contact lens options with new designs might bring better life quality for patients with severe keratoconus.
Contemporary contact lens management of keratoconus is no longer limited to the use of corneal rigid gas permeable lenses. Alternatives today also include
specialty keratoconus soft lenses, vaulting hybrid lenses, scleral GP lenses as well as tandem/piggyback lens systems. The advantages of these other
alternatives to corneal GPs includes significant improvement in lens comfort, minimization of lens to cornea direct contact, improved lens positioning and
fit stability all the while still maintaining excellent visual improvement. The net outcome of the utilization of the various contact lens alternatives can
be a significant improvement in our patient�s quality of life. The question now is �where do we start when it comes to contact lens options for
keratoconus?� If faced with a newly diagnosed case of keratoconus should we initially attempt corneal gas permeable lens fitting or should we consider the
alternatives that we now have access to? Unfortunately other elements can come into play such as expense differences and whether or not third party
coverage for medically necessary contact lenses will allow us to go straight towards the alternatives to corneal GPs. We are already seeing medically
necessary CL plans being introduced that tie reimbursement and lens designs options to the degree of severity of keratoconus. I strongly feel that the
decisions pertaining to the most appropriate CL option for our patients should always be made between the doctor and patient. OK, call me old school!
1. Wu Y, Tan Q, Zhang W, Wang J, Yang B, Ma W, Wang X, Liu L. Rigid gas-permeable contact lens related life quality in keratoconic patients with different
grades of severity.
Exp Optom
. 2014 Dec 29. [Epub ahead of print]
^ Back to top
|
|
|
|
|
 |
OCULAR SURFACE UPDATE
Katherine M. Mastrota, MS, OD, FAAO
|
|
|
|
|
|
|
|
Makeup and Eyelash Structure
One of my colleagues who is as interested in Demodex as I am, recently asked me how the use of makeup impacted, or not, populations of Demodex in and
around the lid margin and how. Frankly, I don�t know. In researching it, I did pick up an interesting tidbit of information:
A recent Japanese study investigated how eye makeup affects the eyelash structure. The internal structure of eyelashes was observed with a scanning X-ray
microscopic tomography system from 36 Japanese women aged 20-70 years and whose use of eye makeup differed.1 Reconstructed cross-sectional
images showed that the structure of the eyelash closely resembled that of scalp hair. The researchers noted that eyelash structure is changed by use of eye
makeup. There was a positive correlation between the frequency of mascara use and the degree of cracking in the lash cuticle (the hard 5-12 layer deep
surface shingle-like layer of dead, overlapping cells which gives the hair shaft strength). Positive correlation was also found between the frequency of
mascara use and the porosity of the cortex (the cortex of the hair shaft is located between the hair cuticle and the innermost medulla and is the thickest
hair layer; it contains most of the hair�s pigment, giving the hair its color).
I wonder if/how lashes, perhaps compromised by mascara, impact Demodex populations. Would they be more or less �comfortable� in a sub-par hair environment?
Does the mascara impact the eyelashes only, or does it affect the follicle that the hair is generated and resides in? What about the hair stem cell
environment? So many questions�
Fukami K, Inoue T, Kawai T, Takeuchi A, Uesugi K, Suzuki Y. Internal structure changes of eyelash induced by eye makeup. J Cosmet Sci. 2014
Jul-Aug;65(4):217-24.
^ Back to top
|
|
|

|
|
Seasonal, Geographic, and Antimicrobial Resistance Patterns in Microbial Keratitis: 4-Year Experience in Eastern Pennsylvania
|
|
The aim of this study was to review the demographics, causative organisms, seasonal and geographic variation, and antimicrobial resistance patterns of
microbial keratitis at the researchers' institution over a 4-year period.
Electronic medical records of all patients with microbial keratitis who underwent corneal culturing at a single institution in eastern Pennsylvania between
January 1, 2009 and December 31, 2012 were reviewed.
A total of 311 patients representing 323 instances of infectious keratitis were analyzed. The most frequently implicated organisms in contact lens-related
infections were Pseudomonas aeruginosa for bacteria and Fusarium species for fungus, compared with Staphylococcus aureus and Candida species in non-contact lens-associated bacterial infections. Bacterial keratitis occurred most frequently in spring and least frequently
in winter (P = 0.024). Patients who live in large fringe metro (suburban) areas accounted for the highest proportion of infectious keratitis cases.P. aeruginosa and methicillin-sensitive S. aureus isolates were highly susceptible to fluoroquinolones, whereas 32% of coagulase-negative staphylococcus isolates tested were resistant to moxifloxacin and gatifloxacin, and all methicillin-resistant S. aureus organisms tested
were resistant to these two fluoroquinolones. No organisms tested were resistant to tobramycin, gentamicin, or vancomycin. No fungal infections tested were
resistant to voriconazole.
The authors concluded that most infectious keratitis occurred in non-winter months and in patients from suburban counties. Although fluoroquinolones were
effective against the most common bacteria, staphylococcal species exhibited a high rate of resistance, representing a therapeutic challenge given the
increasing use of fluoroquinolones as first-line monotherapy. No organisms tested were resistant to tobramycin, gentamicin, vancomycin, or voriconazole.
Ni N, Nam EM, Hammersmith KM, Nagra PK, Azari AA, Leiby BE, Dai Y, Cabrera FA, Ma JF, Lambert CE Jr, Honig SE, Rapuano CJ. Seasonal, Geographic, and
Antimicrobial Resistance Patterns in Microbial Keratitis: 4-Year Experience in Eastern Pennsylvania. Cornea. 2015 Jan 19. [Epub ahead of print]
|
|
|
|
|
|
A Proud Supporter of

Important Links:
To report adverse contact lens reactions visit:
http://www.accessdata.fda.gov/scripts/medwatch/ or call (800) FDA-1088.
To report possible grievances related to the Fairness to Contact Lens Consumers
Act or associated Contact Lens Rule visit:
https://www.ftccomplaintassistant.gov/.
CLToday Services:
Subscribe;
Unsubscribe; Submit Clinical
Image
Submit news to cltoday@pentavisionmedia.com.
Send your comments and fitting tips to
cltoday@pentavisionmedia.com. Please include your full name, degree or title
and city/state/country.
For more information on Contact Lenses Today including archives of previous
issues, please visit our website at www.cltoday.com.
For the latest articles on contact lenses, important clinical information and helpful
tools related to the contact lens practice visit the Contact Lens Spectrum
website at www.clspectrum.com.
© 2015 All Rights Reserved Contact Lenses Today and CLToday
are registered trademarks of:
PentaVision LLC, 321 Norristown Road, Suite 150, Ambler, PA 19002 | 215-628-6550
© 2015 PentaVision LLC All Rights Reserved.
|
|
|
|
|